DOI: 10.1097/PRS.0000000000012812
Polydioxanone (PDO) Thread Lift for Face: A Novel Anatomical Approach
Arthur Y. Yu, MD, PhD and Lee L. Q. Pu, MD, PhD
Corresponding author information: Arthur Y. Yu, MD, PhD Premier Cosmetic Surgery &
MedSpa 59 Las Tunas Dr. Arcadia, CA 91007, USA Tel. 1-626-285-0508 Cell: 1-626-548-1219
Email: ayyy888@gmail.com Instagram: dr.arthuryu; Co-author: Lee L.Q. Pu, MD, PhD
University of California Irvine and University of California Davis New Port Plastic Surgery
20301 SW Birch St, Ste 100, Newport Beach, CA 92660 ·Email: llpu@ucdavis.edu
Financial disclosure and conflict of interest: Arthur Y. Yu have nothing to disclose and has
absolutely no conflict of interest. Dr. Lee L. Q. Pu has received royalties from Thieme and
Elsevier for his published books and issues of Clinics in Plastic Surgery.
Short running head: “A novel face PDO thread lift technique”
Part of this work was presented in the 2023 AMWC Americas Conference, Miami, FL, the
2024 Plastic Surgery the Meeting, San Diego, CA, and the 2025 International Society of
Plastic Surgeons (ISAPS) Conference, Singapore. Polydioxanone (PDO) Thread Facelift: A Novel Anatomical Approach
This is an open-access article distributed under the terms of the Creative Commons AttributionNon Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal.
Barbed thread facelift has grown in popularity, however, optimal strategies for thread placement remain inconclusive. Currently, most practitioners use cannula-driven method for thread facelifts. However, the lifts are generally performed without firm anchors, and many cephalad barbs remain unused. These methods could result in differing degrees of clinical effectiveness. This paper proposes a novel technique using molded polydioxanone (PDO) threads for facial rejuvenation. For midface lift, PDO threads attach to the zygomatico-cutaneous ligaments (ZCL) and anchor to the superficial layer of the deep temporal fascia (SDTF) using a bi-directional threading technique. For buccal fat ptosis and lower face lift, we use threads to engage the buccal fat complex and hitch it at the sideburn region. Additional improvement of jowling is also attained by utilizing the platysma auricular ligament. We have performed this procedure in 83 patients with minimal complications. The engagement of ZCL and buccal fat, along with solid thread anchoring and utilization of all barbs, allows for effective mid and lower face elevation with favorable aesthetic outcomes. The results appear natural, and patient’s satisfaction is high. This method applies long-standing plastic surgery concepts to achieve enhanced thread lifting effects. Even though PDO thread facelifts only produce temporary effects, they provide an option for patients who are hesitant about surgical facelifts.
Thread-lifts have become more and more popular in the past two decades, but needledriven techniques face technical barriers,1,2 and cannula methods often lack solid anchors (Figs. 1 and 2). Additional insufficiencies include engagement of random subcutaneous tissues, with possible early thread failure.3-8
We present a technique using PDO threads that targets crucial facial structures, such as the zygomatico-cutaneous ligament (ZCL) and buccal fat, to improve lifting effect and durability, with more solid cephalad anchoring.1
The ZCL, buccal fat and thread insertion vectors are marked (Video, SDC 1). The face is sterilized, and local anesthesia is administered using 0.5% lidocaine with epinephrine. 1) For midface correction, a bi-directional thread deployment method is employed (Fig. 1). An 18G needle is used to create an adit 2 cm lateral and 0.8 cm caudal to the lateral canthus (selecting this landmark optimizes thread-lifting effect while reducing distortion of eyelid anatomies. We did find that this landmark is useful for all races and genders.). Molded PDO thread cannulas (19G, USP size 0, 100 mm, Viola, Brea, CA. (Similar threads are available from most other manufacturers)) are inserted at the deep subcutaneous level, targeting the robust subcutaneous fibers of ZCL.9-11 A “break-through” sensation signifies penetration through the ligaments. After inserting half the cannula with thread deployment, the surgeon withdraws the cannula and redirects it toward the temple, while lifting the midface. The cannula is then bowed up to engage the cannula to the superficial layer of the deep temporal fascia (SDTF) (2–3 threads). The final cannula placement was by gliding along the pre-determined depth and path. If skin bunching occurs, a hairline adit at the peak is made for relay skin-lifting. 2) For buccal fat and lower face lifting,9 a 14G adit is created at the sideburn. Two threads are inserted subcutaneously, crossing the anterior masseteric border. The cannulas are arched upward, directing the tips downward to contact the buccal fat complex. The threads are tied. 3) For correction of the mandibles or jowls, a 14G adit is created behind the earlobe, behind the platysma auricular ligament.12 Two threads are inserted subcutaneously: one, 1 cm above the mandibular border, and another 1 cm below, with knots tied (Fig1- 2; videos, SDC 1-3).
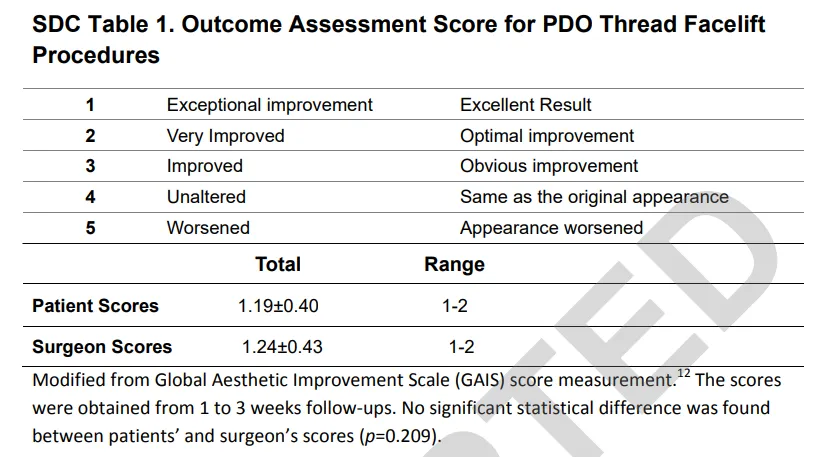
Patients were asked to sit up for adjustments. Extra-strength acetaminophen was prescribed for pain. Follow-ups occurred at 1–3 weeks, 3–6 months, and 6–24 months. Global Aesthetic Improvement Scale (GAIS) was assessed in-person at the initial 1-3 week follow-up (Table, SDC 4; Fig. 3).3,13,14 Subsequent follow-ups were carried out by in-person or messaging method.
This study is retrospective, conducted between June 2020 and May 2024 in accordance with the Declaration of Helsinki. It included 83 Asian female patients aged 27 to 74 (50.17±9.69). Patients considering thread facelift were eligible unless they had very heavy faces or crepey skin. Statistical analysis was performed using Microsoft Excel (Microsoft, Redmond, WA).
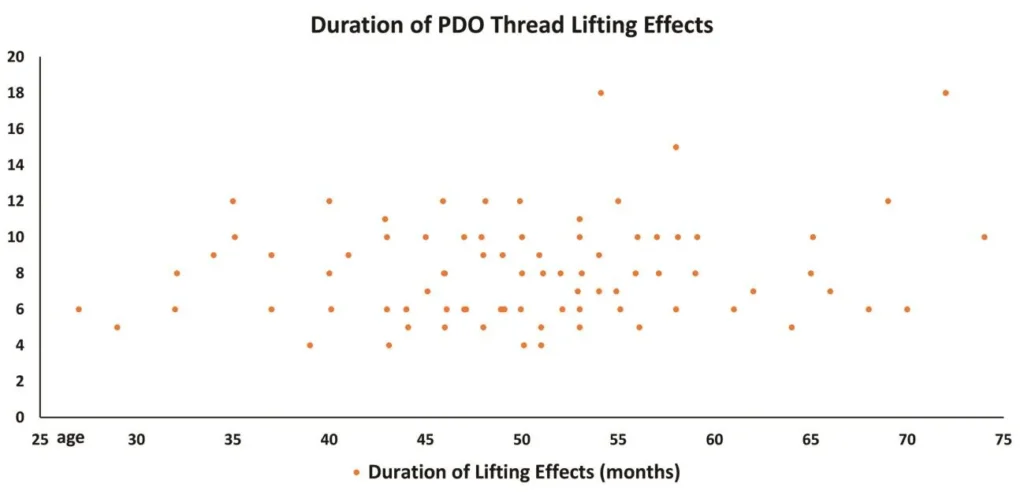
Both patients and the surgeon reported high satisfaction with the results (Table, SDC 4). Patients reported results lasting 4-18 months (8.07±2.84 months). Dimpling appeared in 17 patients but resolved within 1–2 weeks. Three cases of thread extrusion occurred and were treated by thread removal. Bruising (7 cases, 8.43%) and swelling (100%) typically last two weeks. Thirty four patients had recurrent thread-lifts with the results duplicated (41%). Five patients were converted into deep-plane facelifts (6.02%). In 3 cases, the threads remained in place and were positioned within the intended tissue layer(s). There were no significant difficulties in carrying out the deep-plane facelifts.
Progress in thread-lifting has been limited. Most thread-lifts lack solid anchors and do not fully engage all cephalad barbs (Fig. 1), so results could last only 2-6 months, often with suboptimal lifting results.3-7,15-23
ZCL is a thick osteo-cutaneous ligament extending from the zygomatic arch to the medial maxilla, with marked thickening along the zygoma (Fig.2).9,10 A prominent midface aging change is the attenuation of the ZCL with ensuing hanging of the superficial ZCL structure. Lifting superficial ZCL effectively repositions malar fat pads.9-11 Engaging the superficial ZCL with threads does not create a mechanical barrier; rather, it targets the ligament for optimal lifting, analogous to the mechanism observed in deep-plane facelifts. Once the superficial ZCL is engaged, the full length of barbed cephalad threads anchors to the solid SDTF for a more secure midface lift. SDTF thread anchoring was confirmed in 20 ultrasound studies. Due to the toughness of the SDTF and use of a blunt cannula, only the temporoparietal fascia may be breached, rather than the SDTF. This technique is similar to Wu’s needle-driven thread lift, which anchors threads to the deep temporal tissue.¹ The midface lift facilitates subsequent elevation of the buccal fat, with the threads anchored at the sturdy sideburn region. No injury to the buccal branch(es) of the facial nerve was observed. During deep plane facelift procedures on our converted patients, threads were consistently found to lie tangentially to the buccal fat membranes. Utilization of the platysma auricular ligament with thread knotting further helps mandible and jowl improvement (Figs. 1-3; videos and Figures, SDC 2-7).
This technique demonstrates substantial efficacy (Table, SDC 4), with results persisting for 4-18 months (8.07±2.84 months. Figure, SDC 5), exceeding that in prior studies.3,4 Lifting effects less than 5 months may be attributed to factors such as insufficient ligament engagement, 5 cheese-wiring, or tissue relaxation/creeping phenomena.24 Furthermore, the outcomes observed may have been influenced by patients’ interpretations.
A key limitation of this study is the absence of a control group using traditional thread lifting methods. All participants were Asian females, limiting generalizability to other groups. Further, many patients live out of state or abroad, so long-term follow-up often occurs remotely, which is less reliable than in-person assessments. While most patients experience effects beyond 6 months, the corresponding author noted that optimal results usually persist for only 4 to 5 months before tapering off (Figure, SDC 7). Additionally, this report reflects a single institution’s experience.
In summary, established plastic surgery principles regarding ZCL and buccal fat were applied to improve the efficacy and, potentially, the durability of thread lifting procedures. Solid, full thread anchoring on SDTF also helped significantly. The results appear natural and are associated with good patient satisfaction.
Figure 1. The right face illustrates conventional PDO thread placement. The left face demonstrates our new method. Ultrasound study on a real patient was performed with a Clarius Scanner (Model L15, HD3, Vancouver, BC, Canada). The upper panel shows the traveling of the cannula tightly on top of the SDTF, while the lower panel displays the cannula traveling deep in the subcutaneous tissue. The model picture was obtained with full license agreement from Shutterstock (New York, New York). TPF, temporoparietal fascia; DDTF, deep layer of deep temporal fascia.
Figure 2. This figure illustrates the key landmarks on the face for PDO thread placement. The blue dotted line connecting the lateral canthus to the mandibular angle indicates the division point between the mobile and immobile parts of the face.10 The anterior/mobile part is further divided into the ‘catch zone’ (yellow) and ‘non-catch zone’ (brown, nasolabial fold) for thread placement. The green dotted line indicates the lower border of the zygomatic arch and zygoma. The zygomatico-cutaneous ligament (ZCL) can be confirmed by pressing the superior zygomatic skin caudally. A groove will form, indicating tethering on the skin by the ZCL (Horizontally placed blue dots. The thicker the dots, the more robust the ligamentous fibers). The buccal fat can be palpated/pinched and marked (light green).
Figure 3. This 52-year-old female, complaining of a failed surgical facelift from 2 years prior. She stated that the facelift effect only lasted 6 months. She was unwilling to undergo surgeries anymore. PDO thread facelift was performed as described in Fig. 2. One week post procedure, she demonstrated ideal results showing satisfactory correction of nasolabial folds, buccal fat prolapse and jowling. Droopy face appearance and mandibular borders were significantly improved. Even the neck tissues became tightened. She reported that her result lasted 6 months and subtler changes remained for an additional 2 months.
Video, SDC 1. Markings and local anesthesia for PDO thread placement.
Video, SDC 2. Execution of facelift with PDO thread placement. This patient reported her result lasting 12 months.
Video, SDC 3. Bi-directional deployment of a PDO thread using a transparent silicone implant for demonstration purposes.
Table, SDC 4. Global Aesthetic Improvement Scale (GAIS) Assessments.
Figure, SDC 5. Distribution of patient reported durations of thread lift effect
Figure, SDC 6. Frontal view of the same patient as in Fig.3. Left denotes before, and right, one week after the thread lift. The midface became fuller and the lower face slimmer, contributing to the better-defined “V”-shaped face.
Figure, SDC 7. This 50 year-old female, underwent PDO thread placement. Left denotes before the procedure; second to the left shows the result at 3 months; second to the right is at 7 months; and the right, at 16 months.
Figure 1
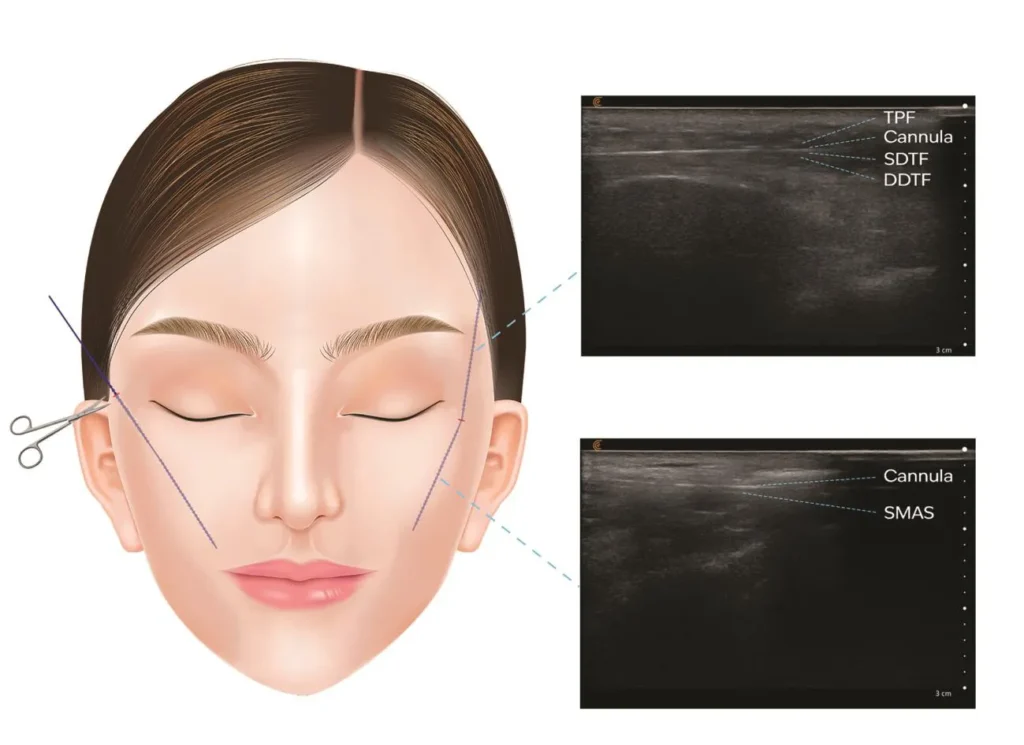
Figure 2

Figure 3A

Figure 3B

SDC Figure 1
SDC Figure 2

SDC Figure 3




